
What Is Hypermobility? Signs, Symptoms & When to See a Physio in Auckland
You have probably heard it your whole life: “You’re so flexible!” Maybe you could do the splits as a kid, or you impress people at parties by bending your thumb back to your wrist. It sounds like a party trick. But for a growing number of people in Auckland and across New Zealand, that same “gift” of flexibility is behind years of unexplained pain, exhaustion, and recurring injuries.
If you find yourself spraining ankles repeatedly, dealing with chronic joint pain, feeling like your body just does not hold together the way it should — there is a real clinical reason for that. And there is a name for it.
Joint hypermobility is a condition where joints move beyond their normal range of motion. In its milder forms, it is simply a structural trait. But in more significant presentations — including Hypermobility Spectrum Disorder (HSD) and hypermobile Ehlers-Danlos Syndrome (hEDS) — it is a systemic connective tissue condition that affects your joints, your muscles, your nervous system, and your quality of life.
At Velca in Howick, we assess and manage hypermobility-related conditions as part of our musculoskeletal services. Here is everything you need to know.
Part 1: What Is Hypermobility?
Your joints are held together by ligaments, tendons, and the joint capsule — essentially a network of connective tissue. In people with hypermobility, this connective tissue is more elastic than it should be. This means joints can extend beyond their normal range of motion, and they may not hold their position reliably under load or during movement.
This is not just about being "double jointed." The problem is not the range of motion itself — it is what that laxity does to the surrounding structures. When ligaments cannot provide adequate joint stability, the muscles have to work overtime to compensate. That leads to fatigue, pain, and injury.
The Beighton Score: The Clinical Measure of Hypermobility
Clinicians use a simple screening tool called the Beighton Score to assess generalised hypermobility. It tests nine specific movements across your hands, elbows, knees, and spine. You score one point for each that exceeds the normal range.
Can you bend your little finger back more than 90°? (1 point each hand)
Can you bend your thumb back to touch your forearm? (1 point each hand)
Do your elbows extend more than 10° beyond straight? (1 point each elbow)
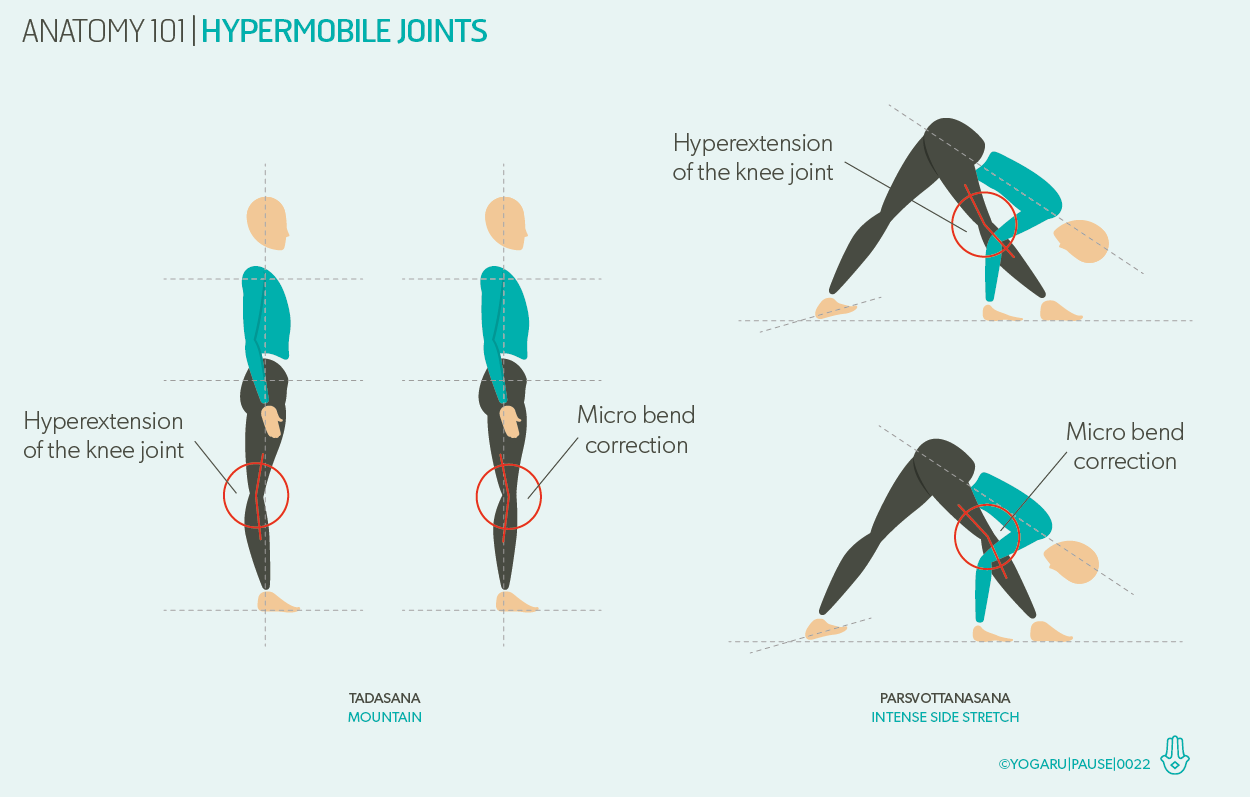
Do your knees extend more than 10° beyond straight? (1 point each knee)
Can you place your palms flat on the floor with straight legs? (1 point)
A score of 4 or more out of 9 in adults suggests generalised hypermobility. But the Beighton Score is just a starting point. Hypermobility is diagnosed clinically, alongside a full symptom history and assessment — not just a single test.
Part 2: Signs and Symptoms — The Ones People Miss
Most people with hypermobility know their joints are "a bit bendy." What they do not always connect is the full picture of symptoms that can accompany it.
Joint-Related Symptoms
Recurring joint sprains or instability — particularly ankles, knees, and wrists
Joint pain that is worse after activity or prolonged sitting/standing
Clicking, popping, or grinding joints (often dismissed as normal)
Joints that feel like they “slip” or partially sublux during everyday movement
Tendon or muscle strains from seemingly minor activities
Systemic Symptoms (Often Overlooked)
This is where many people with hypermobility spend years being told nothing is wrong. The connective tissue that is lax in your joints is the same connective tissue throughout your entire body — including your blood vessels, digestive system, and autonomic nervous system.
Fatigue — often disproportionate to activity level, and not relieved by rest
Dizziness or lightheadedness when standing up (a sign of dysautonomia or POTS-like symptoms)
Poor proprioception — a reduced sense of where your joints are in space, which increases injury risk
Digestive issues including bloating and gut motility problems
Skin that is soft, stretchy, or bruises easily
Anxiety — the autonomic nervous system is often dysregulated in hEDS and HSD
If several of these feel familiar, you are not imagining it. The medical community is increasingly recognising that hypermobility-related conditions are significantly underdiagnosed — particularly in women.
Part 3: HSD vs hEDS — Is There a Difference?
This is one of the most common questions we get at Velca. The short answer: yes, but the distinction matters more for diagnosis than for treatment.
Hypermobility Spectrum Disorder (HSD) is the term used when someone has generalised joint hypermobility with associated symptoms, but does not meet the full diagnostic criteria for hEDS.
Hypermobile Ehlers-Danlos Syndrome (hEDS) is diagnosed using the 2017 International Classification criteria. It requires generalised hypermobility plus additional features: a positive family history, musculoskeletal features (such as chronic pain or recurring subluxations), and at least one systemic manifestation.
The practical reality? Both conditions cause similar problems and respond well to the same physiotherapy approach. What matters clinically is not just the label — it is understanding how hypermobility is affecting your specific body and daily function.
Part 4: Why Does It Matter If Left Unmanaged?
Joint hypermobility is not just about being bendy. When it is not properly managed, it creates a self-reinforcing cycle that gets harder to break over time.
Instability leads to guarding. Your body learns to protect unstable joints by tensing surrounding muscles. This protective tension causes its own pain, and over time leads to stiffness, postural changes, and reduced movement.
Fatigue leads to deconditioning. People with hypermobility often reduce their activity to avoid pain, which weakens the muscles that the joints depend on for support — making instability worse.
Misdiagnosis leads to the wrong treatment. Without a clear hypermobility diagnosis, many patients are treated for isolated conditions — one ankle sprain, one back episode — without ever addressing the underlying connective tissue issue. The injuries keep coming back.
Early, targeted physiotherapy breaks this cycle.
Part 5: When to See a Physio — and What to Expect at Velca
If you recognise yourself in this article, a physiotherapy assessment is the right first step. You do not need a GP referral to book with us at Velca.
What Our Assessment Covers
A thorough joint hypermobility screen using the Beighton Score and additional clinical tests
Assessment of muscle strength, control, and proprioception across key joints
Review of your full symptom picture — including fatigue, autonomic symptoms, and pain patterns
Identification of which joints are most at-risk and what is driving your current pain
What Treatment Looks Like
Physiotherapy for hypermobility is different from standard physio. Stretching is generally not helpful — your tissues are already too lax. The focus instead is on:
Joint stabilisation exercises — building the specific muscle strength needed to protect each vulnerable joint
Proprioceptive training — retraining your nervous system to sense joint position accurately
Load management — helping you stay active without overloading unstable joints
Pacing strategies — particularly important if fatigue is a significant symptom
Education — understanding your body is half the battle. Knowing why something happens makes it far less frightening and far easier to manage.
Most people with hypermobility can lead full, active lives with the right support. The goal at Velca is not to limit what you can do — it is to give you the tools to do it safely and sustainably.
Ready to get answers? Book a physiotherapy assessment at Velca in Howick. Our team will assess your joints, review your full symptom picture, and build a plan specifically for you.